Management of COPD in the UK is based on NICE guidelines and draws on the recommendations and priorities of GOLD. Both say community pharmacists should:
- Offer treatment and support to stop smoking, pulmonary rehabilitation if appropriate and pneumococcal and influenza vaccines
- Co-develop a personalised self-management plan
- Optimise treatment for co-morbidities
- Confirm diagnosis using objective measurements (spirometry following SABA use [post-bronchodilation])
- Assess airflow limitation FEV1/FVC <0.7 at diagnosis or to confirm diagnosis
- Assess symptom risk of an exacerbation.
GOLD no longer refers to asthma and COPD overlap; instead it emphasises that they are different disorders, although they may share some common traits and clinical features (e.g. eosinophilia or some degree of reversibility). Asthma and COPD may co-exist in an individual patient.
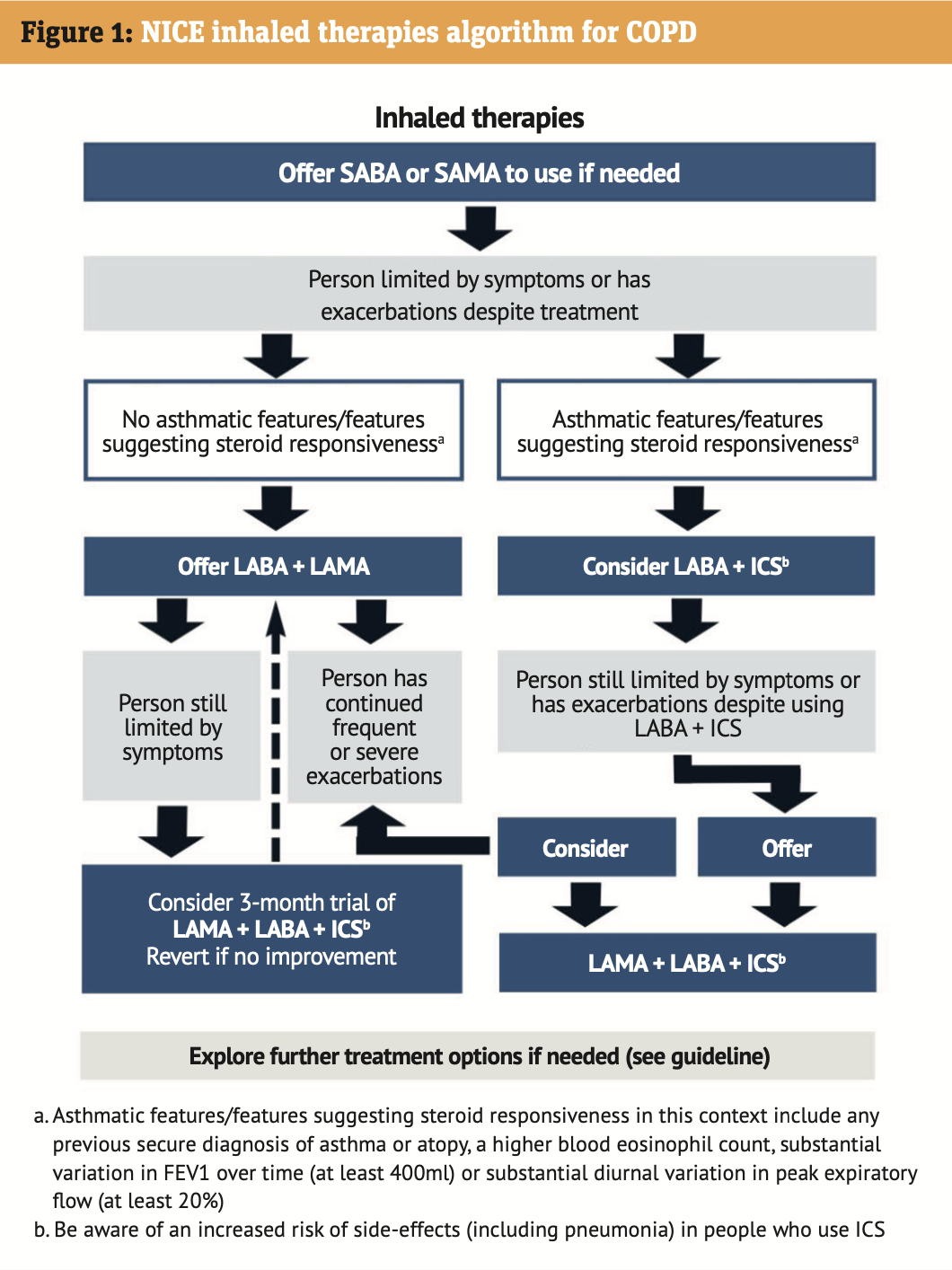
If a concurrent diagnosis of asthma is suspected, pharmacotherapy should primarily follow asthma guidelines, but pharmacological and non-pharmacological approaches may also be needed for the COPD. If and when an inhaled corticosteroid (ICS) should be added to the patient’s treatment is summarised in Figure 1.